アクチノミセス症
アクチノミセスショウ
【英】actinomycosis
=放線菌症
|
放線菌症
ホウセンキンショウ
【英】actinomycosis
【独】Aktinomykose
【仏】actinomycose
同義語:アクチノミセス症
大部分がActinomyces israeliiによる慢性化膿性ないし肉芽腫性感染症である.膿瘍を形成すると,瘻孔が多発し,膿汁が排出される.この膿汁や病巣の中に菌糸が絡み合ってできた菌塊ないし硫黄顆粒sulfur granule,ドルーゼ*Druseがみられる.嫌気性細菌であるA.israeliiは健康人の口腔内に多数生息するもので,本症のほとんどが内因感染である.好発部位は顔・頚部で,胸部,腹部がこれに次ぎ,まれにその他の臓器が侵される.抗生物質時代に入って本症は激減した.顔・頚部型は約半数を占め,菌侵入門戸は歯根膿瘍,う歯などで病変が連続的に波及する.とくに下顎に好発する.徐々に板状硬結をきたし,炎症が表面に及ぶと皮膚は発赤し,やがて赤紫色となり,硬度を増し,表面が凸凹する.ついには軟化し,瘻孔から膿汁が排出し,その中には留針頭大の菌塊をみる.病巣が限局性で,二次感染を伴わない限り局所の疼痛や熱感は軽く,全身状態は比較的良好である.胸部型は歯周囲や扁桃腺窩のActinomyces顆粒を誤飲して起こる.胸痛,せき,痰,発熱があり肺結核や気管支炎に似る.化膿菌との混合感染も少なくない.炎症が進むと胸膜炎,胸膜癒着をきたし,さらに胸壁に及ぶと板状硬結→軟化→瘻孔形成→菌塊を含む膿汁排出へと進行する.腹部型は回盲部に好発し,虫垂炎で始まる.進行すると隣接臓器,腹壁と癒着し,瘻孔を形成する.開腹後診断されることが多い.本病型は事故による受傷者を収容する病院に比較的多い.診断は臨床像と菌塊の証明による.ペニシリンが特効薬で長期大量投与を原則とする.ペニシリン以後,予後は著しく改善された.ときには外科的治療を行う.
|
アクチノミセス症
概要
アクチノミセス症は、Actinomyces 属嫌気性桿菌(主に Actinomyces
israelii)による慢性の化膿性肉芽腫性感染症です。粘膜損傷部位から組織内に浸潤し、周囲に硬結性の腫瘤と多房性の膿瘍を形成します。
病原体
- Gram陽性の分枝状菌(角度のある桿菌)で、嫌気〜通性嫌気性条件下で増殖
- 主に口腔プラーク、歯周ポケット、咽頭粘膜、消化管粘膜、女性の膣内に常在
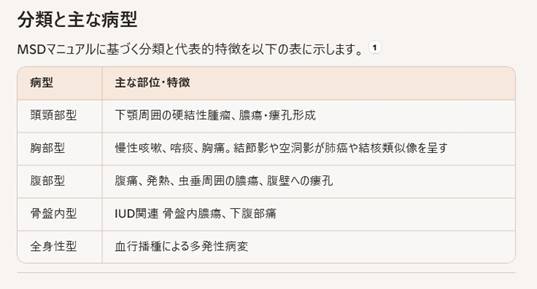
分類と主な病型
MSDマニュアルに基づく分類と代表的特徴を以下の表に示します。
疫学
- 好発年齢は20〜40歳代、成人男性に多い(男女比約3:1)
- 基礎疾患:気管支拡張症、慢性閉塞性肺疾患(COPD)、糖尿病、口腔衛生不良などがリスクを増加
病態生理
- 傷口や粘膜損傷を介して組織内に浸潤
- 肉芽組織、線維化、膿瘍、瘻孔を伴う慢性炎症を呈する
- “硫黄顆粒(sulfur granules)”と呼ばれる黄色円形〜球形の微小膿瘍塊が病理組織学的に特徴的
臨床症状
頭頸部型
胸部型
- 数か月にわたる慢性咳嗽、喀痰、発熱、胸痛
- 肺門部から肺実質内に結節影・空洞影を形成し、肺癌や結核と鑑別困難なことがある
腹部型
- 発熱、腹部痛、しばしば排膿を伴う虫垂周囲膿瘍
- 腹壁への瘻孔形成
骨盤内型
- IUD使用者における下腹部痛
- 骨盤内膿瘍、時に骨盤外への瘻孔
診断
- 画像検査
- 微生物学的検査
- 硫黄顆粒を嫌気培養・グラム染色で確認し、Actinomyces 属を同定
- 病理組織検査
治療
- 抗菌薬療法(最重要)
- 初期:高用量ペニシリン系静注(例:Ampicillin
2 g + 生理食塩水 50 ml 静注 q6 h
2〜6週)
- 継続:Amoxicillin 0.5 g 3〜4回/日 経口投与 6〜12か月
- ペニシリンアレルギー例:テトラサイクリン、マクロライド、クリンダマイシンなどを検討
- 外科的治療
- 大型膿瘍へのドレナージ、瘻孔切除、難治性病変の切除
予後
- 適切な長期抗菌薬治療で数週間以内に症状消失し、完治可能
- 治療中断や診断遅延では周囲組織・骨への浸潤、瘻孔増加、再発リスクが高まる
予防と管理
- 口腔衛生の徹底
- IUD使用者の定期検査および早期交換
- 糖尿病やCOPDなど基礎疾患の適切管理
将来的アプローチ提案
- エージェントベースモデリング(ABM)による組織内感染ダイナミクスのシミュレーション
- 頭頸部型瘻孔に対するマニュアルセラピー(理学療法)を用いた排膿促進効果検証
- 患者由来プラーク中 Actinomyces のオミクス解析で耐性メカニズムや宿主応答の解明
関連文献・ガイドライン
- MSDマニュアル プロフェッショナル版:放線菌症
- 亀田メディカルセンター 呼吸器内科サイト:肺アクチノミセス症
- 日本細菌学会 Actinomyces 白書(PDF)
Main Symptoms of
Actinomycosis
- Cervicofacial involvement
- Indurated, slowly
enlarging mass—often in submandibular or cheek regions
- Formation of sinus
tracts and cutaneous fistulas discharging “sulfur granules”
- Mild to moderate
pain, swelling, occasionally dysphagia or trismus
- Chronic cough with
purulent sputum
- Low-grade fever,
night sweats, weight loss
- Chest pain; imaging
shows nodules or cavitations mimicking tuberculosis or malignancy
- Intermittent fever
and localized abdominal pain (often right lower quadrant)
- Formation of
intra-abdominal abscesses—classically around the appendix
- Sinus tracts to the
abdominal wall with external drainage
- Lower abdominal or
pelvic pain, especially in IUD users
- Pelvic abscesses
and possible fistulas extending to skin or vagina
- Fever, malaise,
sometimes menstrual irregularities
- Disseminated (systemic) spread
- Hematogenous seeding leading to
multifocal abscesses in liver, brain, or bones
- General symptoms: persistent low-grade
fever, weight loss, night sweats
If you’d like more detail
on a specific clinical form, diagnostic approach, or treatment plan, let me
know.
Related topics you might
find useful:
- Diagnostic pearls: sulfur granule
identification, anaerobic cultures, CT/MRI features
- Recommended long-term antibiotic
protocols and alternatives for penicillin allergies
- Surgical indications: abscess drainage,
sinus tract excision
- Emerging research: agent-based modeling
of Actinomyces invasion and host response
- Integrative therapies: manual lymphatic
drainage to support abscess resolution
Direct Answer
Actinomycosis is caused
by normally harmless Actinomyces bacteria breaching mucosal barriers, followed
by chronic, indolent infection driven by anaerobic growth and biofilm
formation.
Pathogen and Host
Interaction
- Gram-positive,
filamentous, branching rods
- Obligate or
facultative anaerobes; form dense biofilms
- Commensal to opportunist shift
- Always present in oral cavity,
gastrointestinal tract, female genital tract
- Require disruption of epithelial
integrity to invade deeper tissues
Key Predisposing Factors
- Mucosal barrier disruption
- Dental procedures
(extractions, root canals)
- Oral trauma: lip
piercings, mucosal ulcers
- Gastrointestinal
perforations: appendicitis, diverticulitis, surgery
- Long-term
intrauterine device (IUD) use
- Local microbiome synergy
- Co-infection with
anaerobes (Fusobacterium, Bacteroides) enhances tissue invasion
- Biofilm matrix
protection reduces antibiotic penetration
- Host immune and systemic conditions
- Poor oral hygiene, periodontal disease
- Diabetes, malnutrition, chronic lung
disease (COPD)
- Immunosuppression (steroids, HIV)
Pathogenesis Sequence
- Mucosal breach lets Actinomyces enter
submucosal tissue
- Anaerobic conditions permit colony
expansion and biofilm formation
- Chronic inflammation generates fibrotic
masses and abscesses
- Formation of sinus tracts and sulfur
granules as hallmark features
Clinical Correlation by
Form
Beyond the Basics:
Research and Prevention
- Biofilm-targeted therapies: enzymatic
disruption or novel antimicrobials
- Phage therapy against Actinomyces to
prevent sinus tract formation
- Agent-based modeling (ABM) of mucosal
breach and abscess evolution
- Omics profiling of patient-derived
Actinomyces for virulence and resistance markers
- Emphasis on strict oral hygiene protocols
and IUD rotation schedules
If you’re interested in
detailed molecular mechanisms, ABM simulation protocols, or tailored prevention
strategies, let’s dive deeper.